Hydronephrosis
Congenital Urinary Tract Obstruction
Hydronephrosis (derived from Greek: hydro = water, nephros = kidney) refers to the accumulation of fluid (urine) in the drainage system of the kidney – the calyces and renal pelvis (see anatomy section). It may due to obstruction of the normal flow of urine or backflow of urine from the bladder, a condition termed reflux (see reflux, UTI section).
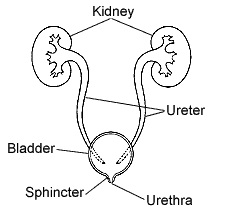
Urine is a filtrate of the blood passing through the kidney and is formed in microscopic units of the kidney called glomeruli. The urine produced in the glomeruli passes from microscopic tubules into larger and visible structures called calyces. Calyces merge to form a renal pelvis which is, itself, connected to the bladder by a long tube called the ureter. When any part of this system is abnormally narrow the flow of urine is restricted and the structure above the area of obstruction distends with urine, very much like a lake forming above a dam.
Because the degree of restriction may vary, the amount of distention or degree of hydronephrosis may also vary. This variability means hydronephrosis may cause serious alterations of kidney function in some circumstances and little or none in others.
Causes of Hydronephrosis
Hydronephrosis can be caused by conditions that the child is born with (congenital) or by conditions that develop after birth (acquired).
The pediatric urologists of Georgia Urology also perform prenatal evaluation if congenital urinary tract obstruction is discovered upon routine imaging during pregnancy.
- Congenital
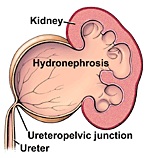
- Ureteropelvic junction obstruction – narrowing of the ureter at the junction between the renal pelvis and ureter
- Ureterovesical junction obstruction – narrowing of the ureter at its insertion into the bladder
- Urethral obstruction – narrowing in the tube leading from the bladder to outside the body (urethra)
Normal Urinary Tract
Ureteropelvic Junction Obstruction
Ureterovesical Junction Obstruction

Acquired
Stricture – narrowing due to the development of scar tissue. This may occur in any part of the drainage system and is most commonly due to trauma or infection
Urinary calculi – Urinary calculi (kidney stones) which are larger than the diameter of the ureter will get stuck and cause a restriction in the flow of urine.
Effects of Hydronephrosis
The effects of hydronephrosis on the kidney are variable. In many cases, mild and sometimes even moderate degrees of hydronephrosis may cause no detectable alteration in kidney function. More severe cases may have caused or may lead to some degree of kidney dysfunction. In some cases, the kidney may have been or could be destroyed by the severity of the condition.
Symptoms of Hydronephrosis
Hydronephrosis may cause no symptoms, even when it is severe. This is particularly true of the congenital forms of hydronephrosis. If the condition leads to urinary infection the child may have fever and pain related to the infection.
Pain – Pain in the flank is the most typical symptom of hydronephrosis. It occurs in most cases of obstruction caused by urinary calculi and in some cases of congenital obstruction. The pain may be severe but is often episodic
Physical Findings
Children with hydronephrosis often have no abnormal findings on physical examination. Some infants with severe hydronephrosis may have abdominal distention or palpable abdominal mass.
Diagnosis of Hydronephrosis
The urinary tract can be imaged with a number of different imaging studies which provide a detailed picture of anatomy and function. Children suspected of having hydronephrosis are often by evaluated with several of these studies:
Renal Ultrasound (RUS): This is usually the first examination. It is readily available, non-invasive and gives a good picture of the size and shape of the kidney. It is particularly good at detecting hydronephrosis
Computerized tomography (CT scan): The CT scanner takes multiple X-ray images of the kidney from multiple angles and collates them into a detailed 2-dimensional image. It gives a precise and detailed picture of the anatomy of the urinary tract. It can be done with and without an intravenously administered contrast agents that are filtered and excreted by the kidney. Because of the multiple images, there is a larger does of ionized radiation than with almost any other imaging study. The CT scan without contrast is particularly good for detecting urinary calculi.
Nuclear Renal Scintigraphy (DTPA, MAG scan): Intravenously administered contrast agents that emit very low levels of radiation and are filtered and excreted by the kidney can be used to evaluate how well, and how rapidly, the kidney filters and excretes waste products. This helps quantify both the degree of obstruction and the effects of obstruction on kidney function.
Voiding Cystourethrogram (VCUG): Reflux of urine can cause hydronephrosis and is detected by dripping contrast into the bladder through a small catheter inserted through the urethra. Once the bladder is full and the child urinates the appearance of contrast in the ureter and/or kidney signifies the presence of reflux
Treatment of Hydronephrosis:
Treatment of hydronephrosis depends on a variety of factors including the cause and severity, symptoms and the effects of the obstruction on kidney function. Generally, efforts to correct the condition would be considered if there are significant symptoms of pain, recurrent urinary tract infection or impairment of kidney function. Some mild cases may cause none of these problems and some cases improve or correct themselves as the child grows.
When symptoms or impaired function indicate a need to correct the blockage and improve the flow of urine the procedure usually involves the surgical excision of the obstruction and re-connection of the un-obstructed drainage tube above and below the blockage. Since most obstructions are short discreet sections of the drainage system this is usually possible.