Recovery, Follow-up, and Prevention
Recovery times vary depending on the age of the patient, the type of treatment performed, and the complexity of the procedure. Discharge from the hospital can be as soon as 1 day to several days after surgery. After treatment, patients are monitored to ensure the ureter remains open and the kidney is draining properly. Follow-up may include imaging studies and routine check-ups.
While temporary and helpful, sometimes stents can cause mild symptoms such as urinary urgency, frequency, or discomfort.
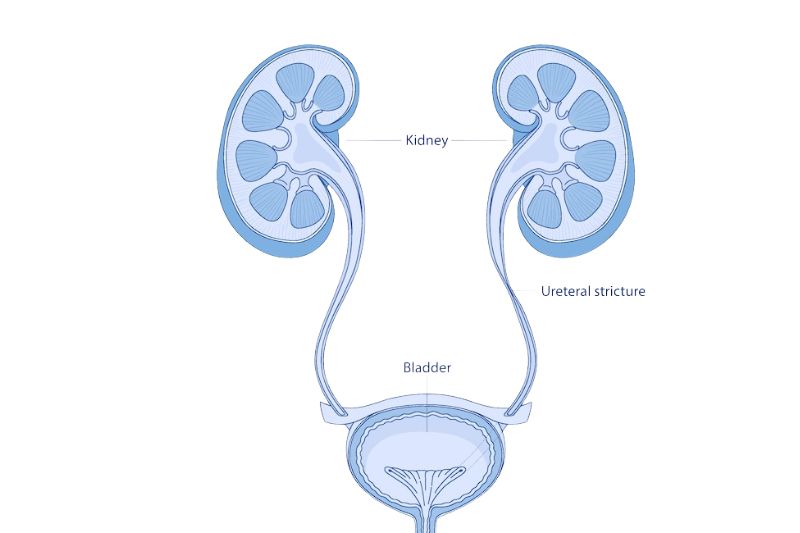
Prevention of ureteral strictures is not always possible, especially in congenital cases, but early treatment of kidney stones, prompt management of infections, and careful monitoring after surgery or radiation therapy may help reduce risk. Prompt attention to urinary retention will also prevent further damage. Narrowing of the ureter can cause renal damage. A severe ureteral stricture can lead to the inability to urinate, which is a medical emergency, as it can lead to hydronephrosis (kidney swelling) and cause the kidneys to stop working (kidney failure).
Georgia Urology is a “Top Doc” independent urology practice, offering exceptional care for men, women, and children. With over 80 providers across more than 30 clinics and ambulatory surgery centers in the Atlanta area, and a 24-hour emergency kidney stone hotline, our goal is to deliver convenient and accessible care to our patients.
FAQs
Will I need surgery?
Not always, as some people may have no symptoms initially. If the stricture is asymptomatic, does not affect kidney function, or is caused by a tumor that responds to other treatments, doctors may opt for observation. Some strictures can be managed with stents, but more severe or persistent cases may require surgical repair.
How serious is a ureteral stricture?
If left untreated, it can lead to kidney damage and become fatal. With proper treatment, outcomes are generally very good.
How long does a ureteral stent stay in place?
Stents may remain in place for weeks to months, depending on the situation, and sometimes require periodic replacement.
Can ureteral strictures come back?
In some cases, strictures can recur, which is why follow-up care is important. Scar tissue that reforms is typically a primary cause.