Physical Findings
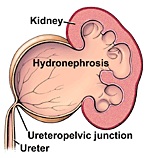
Children with hydronephrosis often have no abnormal findings on physical examination. Some infants with severe hydronephrosis may have abdominal distention or palpable abdominal mass.
Diagnosis of Hydronephrosis
The urinary tract can be imaged with a number of different imaging studies which provide a detailed picture of anatomy and function. Children suspected of having hydronephrosis are often by evaluated with several of these studies:
Renal Ultrasound (RUS): This is usually the first examination. It is readily available, non-invasive and gives a good picture of the size and shape of the kidney. It is particularly good at detecting hydronephrosis.
Computerized tomography (CT scan): The CT scanner takes multiple X-ray images of the kidney from multiple angles and collates them into a detailed 2-dimensional image. It gives a precise and detailed picture of the anatomy of the urinary tract. It can be done with and without intravenously administered contrast agents filtered and excreted by the kidney. Because of the multiple images, there is a larger dose of ionized radiation than with almost any other imaging study. The CT scan without contrast is particularly good for detecting urinary calculi.
Nuclear Renal Scintigraphy (DTPA, MAG scan): Intravenously administered contrast agents that emit very low levels of radiation and are filtered and excreted by the kidney can be used to evaluate how well, and how rapidly, the kidney filters and excretes waste products. This helps quantify both the degree of obstruction and the effects of obstruction on kidney function.
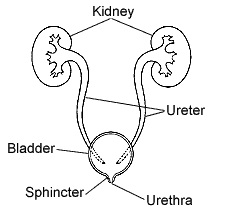
Voiding Cystourethrogram (VCUG): Reflux of urine can cause hydronephrosis and is detected by dripping contrast into the bladder through a small catheter inserted through the urethra. Once the bladder is full and the child urinates the appearance of contrast in the ureter and/or kidney signifies the presence of reflux.
Treatment of Hydronephrosis
Treatment of hydronephrosis depends on various factors, including the cause and severity, symptoms, and the effects of the obstruction on kidney function. Generally, efforts to correct the condition would be considered if there are significant symptoms of pain, recurrent urinary tract infection, or impairment of kidney function. Some mild cases may cause none of these problems, and some cases improve or correct themselves as the child grows.
When symptoms or impaired function indicate a need to correct the blockage and improve the flow of urine, the procedure usually involves the surgical excision of the obstruction and reconnection of the unobstructed drainage tube above and below the blockage. Since most obstructions are short, discreet sections of the drainage system, this is usually possible.