Varicoceles in Children and Adolescents: When and How to Treat?
By Andrew J. Kirsch, MD, FAAP, FACS
Physicians and parents alike are challenged by the management of varicoceles in children. This blog is meant to frame the controversy and educate our patients and families on the current state of the art. As will soon become obvious, shared decision-making is particularly important when considering the many questions that 15% of the male population and their parents need to consider. The first question below is a big question and charged in controversy.
Do adolescent varicoceles have a progressive harmful impact on male fertility?
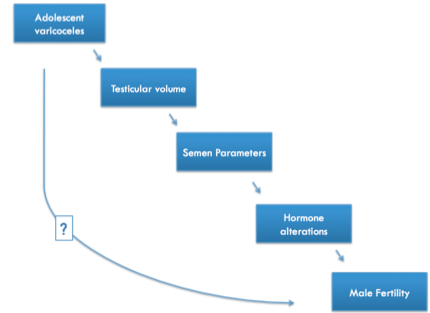
Determining the effect on future fertility is challenging for a variety of reasons
- Limitations in obtaining/interpreting semen analysis
- Unequal differential testicular growth during puberty regardless of varicocele
- A long lag time between varicocelectomy and attempt at paternity
- To add to the confusion, there are no current professional guidelines for children and adolescents
There are 2 main debates among expert pediatric urologists. The first is whether we should treat a varicocele surgically. Here are the issues:
The debate to treat is supported by these facts:
- Varicocele is the most common correctable cause of male infertility
- Corrective surgery (varicocelectomy) improves semen quality
The debate not to treat is also supported by facts:
- Men with varicoceles father children
- Semen quality does not always mean there be a successful pregnancy
The second debate focuses on when to treat a varicocele. Here are the pertinent questions:
Do we treat all adolescents with large varicoceles and smaller testis on the same side? If so, would we overtreat? Or, do we wait and only treat the infertile man trying to start a family? If so, are we too late? Will success be lower? These are the questions that are likely to torment parents of boys with varicoceles.
Here is some data that may help
In the pediatric age patient, the size or volume of the affected (left) testis compared to the normal side is key to helping identify who is at risk for future infertility. Or is it? There are many studies on both sides of this long-standing debate. Larger testis volume differences are associated with significantly lower sperm concentration and motility regardless of patient age or varicocele grade. What is the testis volume loss of boys with varicoceles compared to boys without varicoceles? A study looking at >400 affected boys compared to 70 normal boys showed that those with grade 3 varicoceles had left testis volume loss at all stages of puberty, but also right testicular volume loss compared to controls. In other words, both testes can be affected.
Many studies show that varicoceles are not progressive – they don’t get worse – and catch-up growth occurs without surgery. However, in one study of 100 boys with an average age of 15 years, testicular volume differences > 20% lead to 2x odd of a lower total mobile sperm count. The same study showed total testicular volume (TTV = right + left) <30cc lead to a 4x odds of a lower sperm count. Almost all studies have shown that there does not appear to be any association between testicular volume loss and hormone abnormalities.
So, we have decided that surgery would be the best approach. Is there a difference in outcomes?
When deciding upon differences in surgical approach – laparoscopic (Palomo), microscopic, or open groin incision, there is no good data to support one approach over another. The rates of hydroceles (fluid around testis) or recurrence are generally low (<10%).
Let’s summarize Varicoceles in Children:
The dilemma regarding pediatric varicoceles comes down to these facts:
- Our tools to identify subfertility are imperfect
- Your urologist needs to evaluate all meaningful data
- Testis size (TTV <30cc, TVD >20% )
- Semen analysis when available
- Status of “normal” testis
- Hormone levels (not meaningful in young age)
Parental preference is key. There’s no doubt about it – shared decision-making is critical to the management of varicoceles. Advice to parents: For the majority of boys with varicoceles it makes good sense to follow prospectively and treat conservatively.