Frequently Asked Questions
Q: Who are the candidates for vasectomy reversals?
A: With few exceptions, nearly all vasectomized men are candidates for microscopic reversal procedures, either a vas-vas (vasovasostomy, VV) or a vas-epididymis (epididymovasostomy, EV) connection may be performed. Couples with significant female fertility issues such as fallopian tube blockage or inadequate egg reserve should consider in vitro fertilization (IVF) since the restoration of normal sperm count may not overcome the co-existing female factor.
Q: What are the factors that determine the pregnancy rate following vasectomy reversal?
A: Four major factors are considered in advising individuals regarding the pregnancy rate following vasectomy reversal:
- Obstructive interval or number of years since vasectomy: as reported by the most authoritative study based on the results of 1469 men (VasoVasostomy Study Group, 1991), the pregnancy rates are 76% for reversal performed within 3 years of vasectomy, 53% for 3 to 8 years, 44% for 9 to 14 years and 30% for 15 years or more.
- Age of the female partner: for those couple with the female partners 30 years or younger, this is not likely to be a issue. In a study of 115 couples (Fuch, 2001), the pregnancy rates were 49% with the female age at 31-35, 45% at age 36-40 and 20% at age 41-45. Delivery rates were proportionally lower in the older group as one would expect. Since the success rate is inverse proportional to the passage of time on both partners’ part, the consensus is to proceed with vasectomy reversal sooner rather than later if the decision has been made.
- The use of an operating microscope: the disuse of an operating microscope in the performance of vasectomy reversal simply cannot be supported by the literature. The magnification required to achieve precise suture placement and accurate alignment cannot be provided by visual aids other than an operating microscope with sufficient magnifying power.
- The surgeon: carefully choosing your urologist simply makes sense; whereas some physicians prefer to emphasize the volume of their practice, our recommendation is to consider fellowship-trained male infertility specialists who are well-versed in all aspects of micro-surgery and fertility-related issues.
Q: How involved is the surgery, and what’s the recovery like?
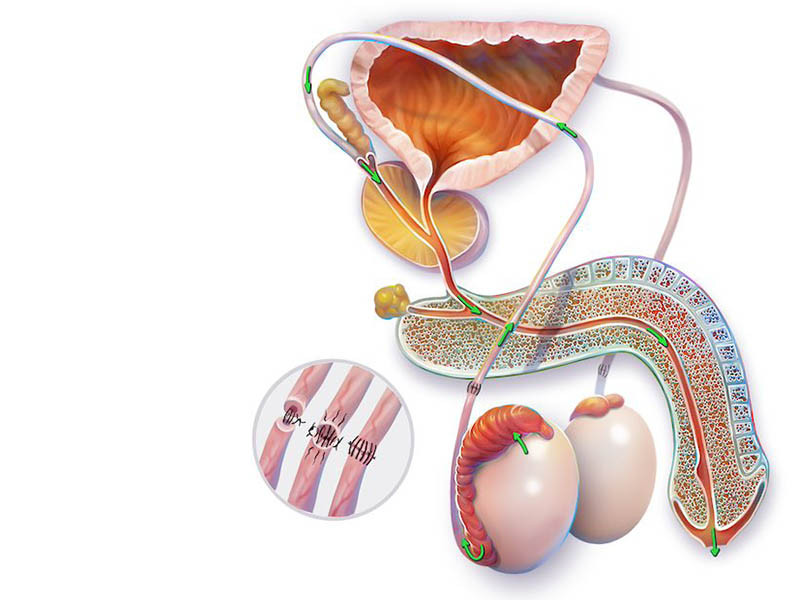
A: For routine reversal or VV, two one-inch incisions are made high in the scrotum. The amount of dissection is limited and you can almost equate the reversal to a “super-sized” vasectomy. The operative time is 2 to 3 hours. For more complicated reversal or EV, the incisions are longer to deliver the testes onto the operative field. A fair amount of tissue swelling is expected post-op. The operative time is 3 to 5 hours since epididymal exploration may be time consuming.
Recovery varies according to the procedure, routine VV is well tolerated with minimal narcotic requirement and one may return to a desk job in 3-5 days. EV is a bit more taxing, one should be prepared to rest for 7 days or more.
Q: What is sperm aspiration?
A: Sperm aspiration in conjunction with in vitro fertilization and sperm injection, IVF/ICSI, is an invaluable tool in the management of infertile couples. Sperm aspiration is done under local anesthesia with a butterfly needle to obtain viable sperm and is inexpensive; however, IVF/ICSI is not. Aspirated sperm are few in number and immature in function, fertilization requires these sperm to be individually injected into each egg in the laboratory. Pregnancy is then established following successful fertilization and embryo transfer to the uterus. Direct insemination is not possible with these sperm and has no role in the management of vasectomized men before reversal.
Q: What is sperm retrieval with reversal?
A: The rationale behind retrieving sperm at the time of reversal is to eliminate the need for future sperm aspiration for IVF if the reversal fails to produce sperm in the ejaculate. The sperm retrieved can only be used for IVF since only a small number of sperm are obtained.
Most men do not require sperm retrieval for the following reasons:
- Routine vaso-vasostomy has a very high patency rate, 80-90% or higher, especially with a short obstructive interval.
- Sperm aspiration is easy and inexpensive; even if the reversal fails, it is no more costly to aspirate sperm later than to retrieve sperm initially. Granted, one does obviate having yet another, albeit minor, procedure done.
On the other hand, the case for retrieval can be made for those undergoing epididymo-vasostomy following extended obstructive interval since the patency will be significantly lower at 50-60%. In these men, we ask them to consider retrieval as an option; some insist on retrieval to avoid any future procedure while others have no problem with a “wait and see” approach.
Sperm may be retrieved by collecting the sperm containing vassal or epididymal fluid or by removing a small piece of testis tissue. The amount of testis removed is about 250 mg, about the size of 2-3 rice grains. It adds very little time to the procedure. Recovery is not much different than reversal.
Arrangements for sperm processing and storage must be made with the andrology lab before the procedure.