My OB Says My Baby Has “Swollen Kidneys”: What is Prenatal Hydronephrosis?
By Shuvro De, M.D.
The 20-week anatomy ultrasound for pregnant moms is one full of anticipation and anxiety, as it sets the stage for the rest of the pregnancy. Prenatal Hydronephrosis is the most common anatomic abnormality found in pregnancy during one of those ultrasounds. It’s found in one percent of all male fetuses and 0.5 percent of female fetuses. Typically, it is not associated with other organ system abnormalities and often the diagnosis does not affect timing or method in which a baby is delivered.
Prenatal intervention is almost never required, and amniotic fluid is usually normal. Depending upon the abnormality, ultrasound imaging may be needed throughout pregnancy and after a baby is born. In most cases, this diagnosis does not affect when, where, or how a baby is delivered. However, surgery is required in a small percentage of children during infancy and childhood.
What is Prenatal Hydronephrosis?
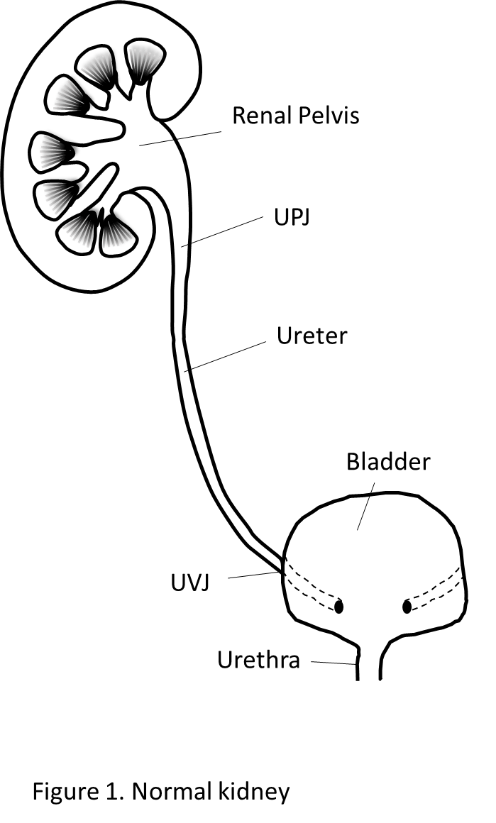 Hydronephrosis is defined as a dilation of renal collecting system—the place where urine is emptied when it is made from the kidneys on its way to the bladder. When urine is made from the kidneys, it first enters a calyx, which then empties into the renal pelvis. Dilation of the renal pelvis can be normal, but dilation of the calyces is typically abnormal.
Hydronephrosis is defined as a dilation of renal collecting system—the place where urine is emptied when it is made from the kidneys on its way to the bladder. When urine is made from the kidneys, it first enters a calyx, which then empties into the renal pelvis. Dilation of the renal pelvis can be normal, but dilation of the calyces is typically abnormal.
When dilation of the renal collecting is found on an ultrasound, a grading system is used to rate the severity of the hydronephrosis. In general, high grade of hydronephrosis at an earlier gestational age is more worrisome than a lower grade of hydronephrosis at a later age.
What Causes It?
Hydronephrosis can be caused by many conditions.
- The first and most common is transient hydronephrosis, which is normal. Since an ultrasound is just a snapshot in time, in transient hydronephrosis the ultrasound captured the kidney when it is maximally full of urine before it drains through the ureter into the bladder. In this situation, multiple ultrasounds show either mild to no hydronephrosis and has no harmful effects for the baby in the future.
- Another cause for hydronephrosis is blockages or partial blockages to the flow of urine, which can occur typically in 3 locations.
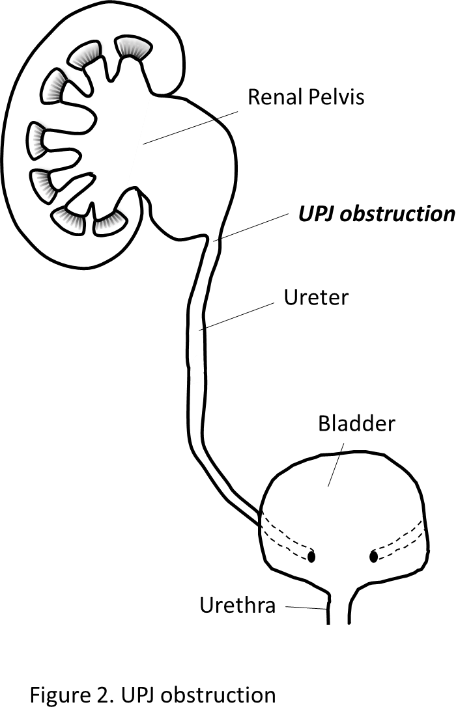
- First, Uretero-Pelvic-Junction (UPJ) Obstruction. It’s a blockage of kidney drainage near the kidney. Depending on the severity of this obstruction, a UPJ obstruction can prevent appropriate kidney development.
- Ureteroceles or other blockages near the Uretero-Vesical Junction (UVJ, where the ureter enters the bladder) a
 re less common causes for hydronephrosis.
re less common causes for hydronephrosis.
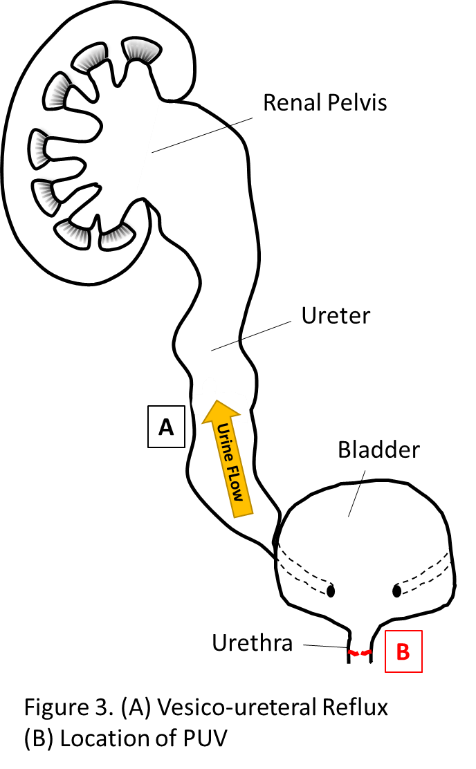
- Most commonly, hydronephrosis is found in one kidney. However, when significant hydronephrosis is found in both kidneys in a boy, the concern is posterior urethral valves (PUV). This is a blockage of urine below the bladder in the urethra. In the womb, urine is critical for the development of the lungs. So, if PUV is present and urine cannot leave the body, lung development can be impaired. Bilateral hydronephrosis in a boy poses a significant concern for urologists and necessitates a multidisciplinary postnatal management team.
- Another cause for hydronephrosis is Vesico-Ureteral Reflux (VUR), which is when urine flows backward from the bladder to the kidney. VUR is most commonly implicated in urinary tract infections with a fever that indicates kidney infections are occurring and potentially leaving scars on the kidney. If the urologists suspect obstruction or reflux, more tests may be needed.
What Do I Do Now?
 In pregnancy, once hydronephrosis is found, it is usually monitored for stability or worsening severity with regular interval sonograms. Prenatal interventions are reserved only for severe bladder outlet obstructions, which is insufficient amniotic fluid with severe obstruction of both kidneys. If this occurs, this would need to be discussed and performed with a multi-disciplinary team. Your obstetrician may send you to a pediatric urologist before your baby is born for more information and establishing care so that plans for after delivery can be made.
In pregnancy, once hydronephrosis is found, it is usually monitored for stability or worsening severity with regular interval sonograms. Prenatal interventions are reserved only for severe bladder outlet obstructions, which is insufficient amniotic fluid with severe obstruction of both kidneys. If this occurs, this would need to be discussed and performed with a multi-disciplinary team. Your obstetrician may send you to a pediatric urologist before your baby is born for more information and establishing care so that plans for after delivery can be made.
Once the baby is born, an ultrasound is usually obtained at 48 hours, which serves as the baseline for future management. Depending on this ultrasound, we may need other tests to determine the specific cause for the hydronephrosis. These tests would tell us which treatment would be best for your child which may include observation with ultrasounds, medications, antibiotic prophylaxis, or surgery.
Do you have any more questions about prenatal hydronephrosis? The experts at Georgia Urology are here to help! Reach out to us by clicking here to schedule a telemedicine appointment.



